Este es un blog medico que nunca podrá sustituir el buen juicio médico en la toma de decisiones.Intentamos compartir con los profesionales nuestras experiencias, conocimientos,lecturas,etc con la finalidad de mejorar la practica clinica.No es un blog para pacientes aunque no rechazamos sus comentarios
Randomized Trial of Nocturnal Oxygen in Chronic Obstructive Pulmonary Disease
Abstract
Background
Long-term oxygen therapy improves survival in patients with chronic obstructive pulmonary disease (COPD) and chronic severe daytime hypoxemia. However, the efficacy of oxygen therapy for the management of isolated nocturnal hypoxemia is uncertain.
Methods
We designed this double-blind, placebo-controlled, randomized trial to determine, in patients with COPD who have nocturnal arterial oxygen desaturation without qualifying for long-term oxygen therapy, whether nocturnal oxygen provided for a period of 3 to 4 years would decrease mortality or the worsening of disease such that patients meet current specifications for long-term oxygen therapy. Patients with an oxygen saturation of less than 90% for at least 30% of the recording time on nocturnal oximetry were assigned, in a 1:1 ratio, to receive either nocturnal oxygen or ambient air from a sham concentrator (placebo). The primary outcome was a composite of death from any cause or a requirement for long-term oxygen therapy as defined by the Nocturnal Oxygen Therapy Trial (NOTT) criteria in the intention-to-treat population.
Results
Recruitment was stopped prematurely because of recruitment and retention difficulties after 243 patients, of a projected 600, had undergone randomization at 28 centers. At 3 years of follow-up, 39.0% of the patients assigned to nocturnal oxygen (48 of 123) and 42.0% of those assigned to placebo (50 of 119) met the NOTT-defined criteria for long-term oxygen therapy or had died (difference, −3.0 percentage points; 95% confidence interval, −15.1 to 9.1).
Conclusions
Our underpowered trial provides no indication that nocturnal oxygen has a positive or negative effect on survival or progression to long-term oxygen therapy in patients with COPD. (Funded by the Canadian Institutes of Health Research; INOX ClinicalTrials.gov number, NCT01044628.)
QUICK TAKE VIDEO SUMMARYNocturnal Oxygen in COPD 01:45
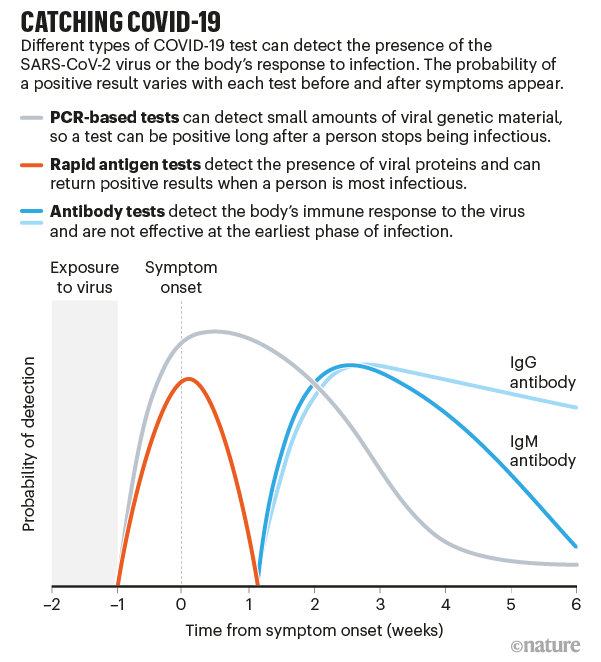
Fast coronavirus tests: what they can and can't do
Rapid antigen tests are designed to tell in a few minutes whether someone is infectious. Will they be game changers?
NEWS FEATURE
Giorgia Guglielmi
Health-care workers test a resident of Mumbai, India, for coronavirus infection using a rapid antigen assay.Credit: Anshuman Poyrekar/Hindustan Times via Getty
The United States leads the world in COVID-19 deaths but lags behind many countries — both large and small — in testing capacity. That could soon change.
At the end of August, the US Food and Drug Administration (FDA) granted emergency-use approval to a new credit-card-sized testing device for the coronavirus that costs US$5, gives results in 15 minutes and doesn't require a laboratory or a machine for processing. The United States is spending $760 million on 150 million of these tests from health-care company Abbott Laboratories, headquartered in Abbott Park, Illinois, which plans to ramp up production to 50 million per month in October.
The tests detect specific proteins — known as antigens — on the surface of the virus, and can identify people who are at the peak of infection, when virus levels in the body are likely to be high. Proponents argue that this could be a game changer. Antigen tests could help to keep the pandemic at bay, because they can be rolled out in vast numbers and can spot those who are at greatest risk of spreading the disease. These tests are also a key element in the testing strategies of other countries, such as India and Italy.
Antigen assays are much faster and cheaper than the gold-standard tests that detect viral RNA using a technique called the polymerase chain reaction (PCR). But antigen tests aren't as sensitive as the PCR versions, which can pick up minuscule amounts of the SARS-CoV-2 virus that causes COVID-19.
This difference raises some concerns among specialists, who worry that antigen tests will miss infectious people and result in outbreaks in countries that have largely controlled coronavirus transmission. Others view the lower sensitivity as an attribute, because some people who receive positive PCR test results are infected, but are no longer able to spread the virus to others. So antigen tests could shift the focus to identifying the most infectious people.
At present, antigen tests are administered by trained professionals, but some companies are developing versions that are simple enough to be used at home — similar to pregnancy tests.
"Making the tests faster, cheaper, easier is definitely the goal — and I think the antigen test is the way to get there," says Martin Burke, a chemist at the University of Illinois at Urbana-Champaign, who is co-developing rapid tests, including antigen-based assays. "This is by no means the perfect solution, it's just the fastest thing we could get going now," he says.
What tests are there and how do they work?
Tests for COVID-19 fall into two categories: diagnostic tests such as PCR and antigen assays, which detect parts of the SARS-CoV-2 virus, and antibody tests that sense molecules that people produce when they have been infected by the virus. Antibodies can take several days to develop after an infection and often stay in the blood for weeks after recovery, so antibody tests have limited use in diagnosis (see 'Catching COVID-19').
Source: Ref. 2
The high-sensitivity PCR tests are almost 100% accurate in spotting infected people, when they are administered properly. But such tests generally require trained personnel, specific reagents and expensive machines that take hours to provide results.
Countries such as South Korea and New Zealand have succeeded in boosting PCR-based testing, but scaling up these tests has proved difficult elsewhere. The United States, for example, has seen a slow and poorly coordinated response to outbreaks, faulty tests from the Centers for Disease Control and Prevention (CDC) and problems with the supply chain. All of this has hindered efforts to collect and process samples for PCR, pushing waiting times to days or even weeks. These delays, along with a lack of tests, have contributed to the rampant spread of COVID-19 across the country, which by 16 September had seen almost 200,000 deaths from the disease.
A typical antigen test starts with a health-care professional swabbing the back of a person's nose or throat — although companies are developing kits that use saliva samples, which are easier and safer to collect than a swab. The sample is then mixed with a solution that breaks the virus open and frees specific viral proteins. The mix is added to a paper strip that contains an antibody tailored to bind to these proteins, if they're present in the solution. A positive test result can be detected either as a fluorescent glow or as a dark band on the paper strip.
Antigen tests give results in less than 30 minutes, don't have to be processed in a lab and are cheap to produce. Yet that speed comes with a cost in sensitivity. Whereas a typical PCR test can detect a single molecule of RNA in a microlitre of solution, antigen tests need a sample to contain thousands — probably tens of thousands — of virus particles per microlitre to produce a positive result1. So, if a person has low amounts of virus in their body, the test might give a false-negative result.
When used on people who were positive for SARS-CoV-2 in a standard PCR test, Abbott's antigen assay correctly spotted the virus in 95–100% of cases if the samples were collected within a week of the onset of symptoms. But that proportion dropped to 75% if samples were taken more than a week after people first showed symptoms. The sensitivity — or the rate of detecting infections correctly — of the other antigen tests used in the United States is between 84% and 98% if a person is tested in the week after showing symptoms.
A technician in a mobile unit conducts rapid antigen tests for COVID-19 in New Delhi.Credit: Mayank Makhija/NurPhoto via Getty
Companies and academic research labs are also rolling out other tests that are faster, cheaper and more user-friendly than standard PCR assays, although they are not being produced on the same scale as antigen tests. Some of these other tests use the gene-editing tool CRISPR to zero in on genetic snippets of the coronavirus. Others are quicker variants of the PCR test that use different reagents, meaning they're not limited by the same supply-chain problems. Saliva-based PCR tests, for example, are being used as screening tools in universities and for professional basketball teams.
Which tests tell whether someone is infectious?
Although the PCR method can test whether someone is infectious, it also detects people who have the virus but are not likely to spread it.
Antigen-based testing, by contrast, could help to rapidly identify people who have high levels of virus — those who are most likely to be infectious to others — and isolate them from the community, says Marion Koopmans, a virologist at the Erasmus University Medical Centre in Rotterdam, the Netherlands. "The question is, what is the safe limit? Because the moment you get that wrong, the whole idea implodes," she says. It's still unclear what viral load is the threshold below which a person is no longer contagious, says Koopmans, who is working with the World Health Organization (WHO) to determine a standard to validate rapid tests. "It would be very worrying if everyone does that on their own, using different criteria," she says.
Viral load peaks early in SARS-CoV-2 infections and then gradually declines, with tiny amounts of virus RNA staying in someone's nose or throat for weeks or possibly months2. And although there are not enough data to equate different viral levels with how infectious people are, there is evidence that individuals are unlikely to spread the virus about eight to ten days after showing symptoms3.
"If you're at risk of transmitting the virus to somebody else, you're going to have plenty of viral particles — those would certainly show up in antigen tests," says Michael Mina, an infectious-disease immunologist at the Harvard T. H. Chan School of Public Health in Boston, Massachusetts, who has been a vocal proponent of antigen tests.
There are challenges at the start of the infection, when people have low levels of the virus. The answer, says Mina, is frequent testing — done multiple times per week. This could quickly identify infected people, even if the assays are less sensitive than a PCR-based test, because the amount of virus in their noses and throats rises within hours, he says.
Mina and his colleagues have used statistical models to assess this strategy. In a preprint updated on 8 September, they suggest that testing people twice a week with a relatively insensitive test could be more effective at curbing the spread of SARS-CoV-2 than are more-accurate tests done once every two weeks1. Another study that modelled different scenarios for safely reopening university campuses reported similar findings4.
To slow outbreaks, the focus should be on identifying those who are at risk of spreading SARS-CoV-2 to other people, rather than on spotting anyone who is infected with it, some experts say.
When used as a screening tool to frequently assess as many people as possible, rapid antigen tests could be "a game changer", says Rebecca Lee Smith, an epidemiologist at the University of Illinois.
How do countries plan to use antigen tests?
At the beginning of April, as coronavirus outbreaks raged across the world, India had tested only about 150,000 people — one of the lowest testing rates per capita worldwide. On 21 August, the country conducted more than one million coronavirus tests in a single day. It reached that milestone after Indian authorities began using antigen assays to boost testing capacity.
Delhi was the first Indian state to begin using rapid antigen tests, in June. By mid-July, the number of cases there had decreased and the daily death counts had plateaued, suggesting that the tests might have played some part in controlling the spread of the virus. Epidemiologist K. Srinath Reddy, president of the Public Health Foundation of India, a non-profit organization in New Delhi, says that the Delhi example is interesting, but not clear-cut: he notes that the government started to lift lockdown restrictions in August, which led to a surge in infections. "Rapid antigen tests have picked up the increased number of cases, but whether they have been successful in limiting the spread of COVID, we'll only know in the next couple of months," Reddy says.
So far, India has approved the use of three antigen tests for screening large numbers of people, whether or not they have symptoms. One of the kits was evaluated by the Indian Council of Medical Research (ICMR) and the All India Institute of Medical Sciences, which found that the test detected infections between 51% and 84% of the time. Guidance from the ICMR says that people who have a negative result from an antigen test should also get a PCR test if they show symptoms, to rule out the possibility that the rapid test missed an infection.
The WHO and the US CDC have also advised getting a PCR test if people showing symptoms test negative with a rapid antigen test. The US FDA has so far granted emergency use authorization for four antigen tests, each of which has a higher sensitivity than those used in India. The 150 million tests bought from Abbott will be used in schools and "other special needs populations", according to the Department of Health and Human Services. The FDA, however, has authorized antigen-based tests only for people who have had symptoms for 12 days or fewer. Tests must be prescribed by a physician and administered by a health-care professional.
A testing centre at the international airport in Rome. Italy plans to use rapid antigen tests to screen passengers at all of its airports.Credit: Simona Granati/Corbis/Getty
Other countries are also considering the use of rapid antigen tests to meet targets. In July, the Philippine Society for Microbiology and Infectious Diseases issued temporary guidelines for clinicians and health-care workers, saying that antigen tests could be used as an alternative to PCR for diagnosing a coronavirus infection during the first week in people with symptoms. But it also recommends that all negative results should be confirmed with a PCR-based assay, says Edsel Salvaña, an infectious-diseases expert at the University of the Philippines Manila, who is advising Philippine officials on rapid testing.
Antigen-based tests are being used in some of Italy's major airports to screen people who arrive from four Mediterranean countries considered to have a high risk of infection. Negative results do not have to be confirmed with a PCR test. The Italian health minister, Roberto Speranza, has announced plans to use antigen tests to screen passengers at all of the country's airports, and a group of experts has urged the Italian government to use the rapid tests in schools and universities.
But others don't think rapid antigen tests are a good idea. When trying to contain small outbreaks, such as those happening in Italy, public-health authorities should use assays that are highly accurate, because missing even just one positive individual could lead to a steep increase in the total number of cases, says Andrea Crisanti, a microbiologist at the University of Padua.
Some researchers worry that there won't be enough antigen tests available to greatly expand their use. "Rapid tests right now are for the happy few," Koopmans says. "If we want to take these assays responsibly forward, we should talk about whether they can be produced to levels that would make them globally available."
Could antigen assays be used at home like pregnancy tests?
Several experts have promoted the idea of developing an antigen test that is cheap and simple enough to use at home, without a health-care worker administering it.
Burke says what's needed is something as easy as a pregnancy test. "You just spit into a tube, put a piece of paper in it and you get the result within minutes," Burke says. "Testing should become a part of life: in the morning you take your cereals, your vitamins, and you quickly check your status," he says.
A few companies are developing simple paper-strip antigen tests. But drug regulators have not yet approved them for emergency use. "We don't have a lot of real-life experience with these tests, and a lot of the validations have only been done in the laboratory," Salvaña says.
Beyond concerns about costs and availability, researchers worry that, with an over-the-counter test, people who get positive results might not follow up with public-health authorities, so their contacts won't be traced. Another risk would be people "gaming the system", Smith says — for example, getting someone else to take their test — so they can be sure of a negative result and avoid quarantine. Without incentives such as freely available tests and a living salary for those who have to isolate, testing and self-isolation could become a luxury reserved for wealthier people, others have argued.
Another concern is that people will get a false sense of security from tests that have only limited accuracy. "There's a big risk that the moment these tests become widely available, people will just use them and say, 'It's negative, so I'm clear,'" Koopmans says.
Even when testing negative, people should continue to wash their hands, wear masks and avoid gathering in big groups, she says. Testing, she adds, "cannot replace the basic control measures that need to be in place to keep this virus controlled".
High admission viral load predicts mortality in hospitalized patients with and without cancer
Patients with cancer may be at increased risk of severe coronavirus disease 2019 (COVID-19), but the role of viral load on this risk is unknown. We measured SARS-CoV-2 viral load using cycle threshold (CT) values from reverse transcription-polymerase chain reaction assays applied to nasopharyngeal swab specimens in 100 patients with cancer and 2914 without cancer who were admitted to three New York City hospitals. Overall, the in-hospital mortality rate was 38.8% among patients with a high viral load, 24.1% among patients with a medium viral load, and 15.3% among patients with a low viral load (P<0.001). Similar findings were observed in patients with cancer (high, 45.2% mortality; medium, 28.0%; low, 12.1%; P=0.008). Patients with hematologic malignancies had higher median viral loads (CT=25.0) than patients without cancer (CT=29.2; P=0.0039). SARS-CoV-2 viral load results may offer vital prognostic information for patients with and without cancer who are hospitalized with COVID-19.
On 3 September The BMJ hosted an online webinar on the diagnosis, management, and prognosis of "long covid." An expert panel discussed its symptoms, course, and character and suggested strategies for managing it. Nikki Nabavi reports
Definition
Panel member Nisreen Alwan (box 1) began the discussion by defining long covid as "not recovering [for] several weeks or months following the start of symptoms that were suggestive of covid, whether you were tested or not."
Box 1
The webinar's expert panel
Nisreen Alwan—associate professor in public health, University of Southampton, and honorary consultant in public health, University Hospital Southampton NHS Foundation Trust. Has personal experience of long covid
Paul Garner—professor, Centre for Evidence Synthesis for Global Health, Liverpool School of Tropical Medicine, and coordinating editor, Cochrane Infectious Disease Group. He has personal experience of long covid
Fiona Godlee—editor in chief, The BMJ (chair)
Trisha Greenhalgh—professor of primary healthcare, Nuffield Department of Primary Care Health Sciences, University of Oxford, and practising GP
Nick Peters—professor of cardiology, Imperial College London, and consultant cardiologist
Valentina Puntmann—senior clinical investigator in cardiovascular imaging, University Hospital, Frankfurt
Tim Spector—professor of genetic epidemiology, King's College London, and leader of the Covid Symptoms Study
RETURN TO TEXT
"Profound fatigue" was a common symptom in most people with long covid, she said, but added that a wide range of other symptoms included cough, breathlessness, muscle and body aches, and chest heaviness or pressure, but also skin rashes, palpitations, fever, headache, diarrhoea, and pins and needles. "A very common feature is the relapsing, remitting nature of the illness, where you feel as though you've recovered, then it hits you back," she said.
Nick Peters added to this definition by highlighting a "distinction between very sick people who have recovered to an extent and [and have been] left with some impact of their severe sickness, versus those who had a relatively mild sickness from the start, in whom it is ongoing."
Alwan described the fluctuations of her own illness: "It's a constant cycle of disappointment, not just to you but people around you, who really want you to recover."
Paul Garner, who also has long covid, described it as a "very bizarre disease" that had left him feeling "repeatedly battered the first two months" and then experiencing lesser episodes in the subsequent four months with continual fatigue. "Navigating help is really difficult," he said.
Tim Spector said that his team at the Covid Symptom Study had identified six clusters of symptoms for covid-19,1 a couple of which were associated with longer term symptoms, indicating a possible way of predicting early on what might occur. "If you've got a persistent cough, hoarse voice, headache, diarrhoea, skipping meals, and shortness of breath in the first week, you are two to three times more likely to get longer term symptoms," he said.
He said that patterns in the team's data suggested that long covid was about twice as common in women as in men and that the average age of someone presenting with it was about four years older than people who had what might be termed as "short covid."
But Spector added, "We do seem to be getting different symptom clusters in different ages, so it could be that there is a different type in younger people compared with the over 65s. As we get more data we should be able to break it into these groups and work out what is going on … which could be very interesting and help us to get early interventions for those at-risk groups."
Peters said that the data showed fatigue was the most common trait in people who had symptoms beyond three weeks. He also said that around 80% of people who had symptoms lasting more than three weeks reported "having had clear good days and bad days."
Cardiovascular effects
Valentina Puntmann, who coauthored a research paper in JAMA Cardiology examining the cardiovascular effects in unselected patients with covid-19,2 discussed one of the study's findings: the relatively high frequency of postviral or inflammatory myocarditis in people who have had covid-19.
She said, "We were all focusing on the lungs and respiratory symptoms to begin with, but the virus attacks the same receptor that is in the heart too, not just the lungs. Many patients who have had heart failure in the past who have now been very unwell with covid symptoms have sustained arrhythmias, meaning their hearts were beating very fast whilst they were ill, and they then went on to develop heart failure.
"If you have pre-existing cardiac conditions, and cardiomyocytes express the ACE2 receptor that the covid virus likes, you are more likely to develop the cardiac symptoms. Taking ACE inhibitors can be used as a preventive measure."
Puntmann said that the illness was "obviously a huge stress on the heart, particularly for those with pre-existing conditions, which can lead to hypoxia and ischaemia of the heart. The clinical course of covid-19 is also much worse in individuals with a troponin leak."
Management
Alwan explained that as someone with long covid "you learn your patterns, learn what brings on utter exhaustion or the other symptoms, and try to avoid those things."
She added, "I'm fairly driven, and I thought I could beat this virus. A friend told me to stop dominating the virus and start accommodating it. Once you start accepting that, it becomes a bit easier. You have to drop your baseline by 90%; you are a different person."
Trisha Greenhalgh said that although many patients referred to long covid clinics were slowly getting better, some were not and urgently needed referring from primary care.
"It should be a story of gradual improvement, and if it's not, consider referring," she advised. She added, "The interface between the GP and the specialist investigations and monitoring is something we have to work on."
Greenhalgh and Matthew Knight, a respiratory physician who ran a clinic for people recovering from long covid, coauthored a recent BMJ article on the management of post-acute covid-19 in primary care.3 A major purpose of the paper, she said, was to reassure GPs that they have the clinical skills to manage these people, such as "listening to the patient, documenting what the symptoms are, how they change and how they fluctuate, and being alert to symptoms that might suggest they need referring."
More broadly, Alwan said that long covid cases should be incorporated into covid-19 statistics. "We are missing a huge opportunity to quantify and measure long covid in the same way that we're doing with positive test results and deaths," she said.
Garner called for research specialists to work together to create better guidance on how to improve investigation in patients with enduring symptoms. "We need rapid interdisciplinary communication," he said.
This article is made freely available for use in accordance with BMJ's website terms and conditions for the duration of the covid-19 pandemic or until otherwise determined by BMJ. You may use, download and print the article for any lawful, non-commercial purpose (including text and data mining) provided that all copyright notices and trade marks are retained.
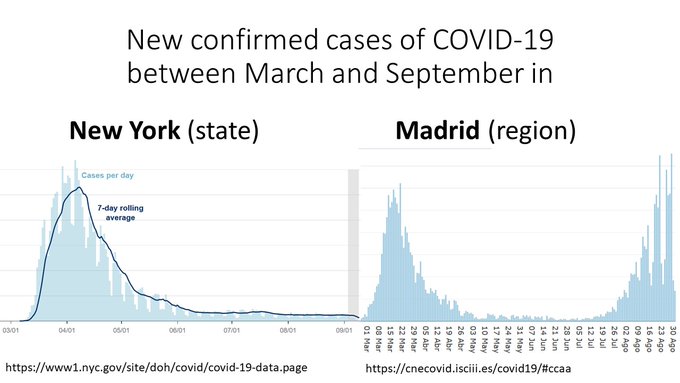
Look at the shape of these curves.
New York and Madrid had similar epidemics until they spectacularly diverged.
In March, both cities were caught by surprise and shut down because of #COVID19.
In September, the situation is under control in NY and alarming in Madrid.
Why?
In summary, we conclude that the relatively transmissibility of asymptomatic case could be significantly smaller than that of the symptomatic cases. The main contribution of Chen et al. (2020) is that they raise the alarm of the existence of the transmissibility of the asymptomatic cases. We remark that how efficient of the transmissibility of asymptomatic cases comparing to symptomatic cases warrants more study.
"A Menace to the Public Health" — Contact Tracing and the Limits of Persuasion
Many countries have been recruiting Covid-19 contact tracers as part of a "test, track, and trace" strategy. In the United Kingdom and the United States, for example, large corps of volunteers have signed up for online classes on the concepts and methods that have served South Korea, Singapore, and Taiwan throughout the pandemic.
Saliva or Nasopharyngeal Swab Specimens for Detection of SARS-CoV-2
Recent studies have shown that SARS-CoV-2 can be detected in the saliva of asymptomatic persons and outpatients.1-3 We therefore screened 495 asymptomatic health care workers who provided written informed consent to participate in our prospective study, and we used RT-qPCR to test both saliva and nasopharyngeal samples obtained from these persons. We detected SARS-CoV-2 RNA in saliva specimens obtained from 13 persons who did not report any symptoms at or before the time of sample collection. Of these 13 health care workers, 9 had collected matched nasopharyngeal swab specimens by themselves on the same day, and 7 of these specimens tested negative (Fig. S2). The diagnosis in the 13 health care workers with positive saliva specimens was later confirmed in diagnostic testing of additional nasopharyngeal samples by a CLIA (Clinical Laboratory Improvement Amendments of 1988)–certified laboratory.
Telemonitoring for Patients With COVID-19: Recommendations for Design and Implementation
Despite significant efforts, the COVID-19 pandemic has put enormous pressure on health care systems around the world, threatening the quality of patient care. Telemonitoring offers the opportunity to carefully monitor patients with a confirmed or suspected case of COVID-19 from home and allows for the timely identification of worsening symptoms. Additionally, it may decrease the number of hospital visits and admissions, thereby reducing the use of scarce resources, optimizing health care capacity, and minimizing the risk of viral transmission. In this paper, we present a COVID-19 telemonitoring care pathway developed at a tertiary care hospital in the Netherlands, which combined the monitoring of vital parameters with video consultations for adequate clinical assessment. Additionally, we report a series of medical, scientific, organizational, and ethical recommendations that may be used as a guide for the design and implementation of telemonitoring pathways for COVID-19 and other diseases worldwide.