Este es un blog medico que nunca podrá sustituir el buen juicio médico en la toma de decisiones.Intentamos compartir con los profesionales nuestras experiencias, conocimientos,lecturas,etc con la finalidad de mejorar la practica clinica.No es un blog para pacientes aunque no rechazamos sus comentarios
Association between duration of use of pharmacotherapy and smoking cessation: findings from a national survey
Results
Sample characteristics and bivariate associations
Weighted sample characteristics are shown in table 1. About 66.7% of the sample reported to have made an unassisted quit attempt; 10% used only prescription medication; 1.1% used prescription medication plus behavioural counselling; 18.2% used only NRT; 2.5% used NRT plus behavioural counselling; and 1.3% used only behavioural counselling. When broken down by duration of use, while most of those who used prescription medication did so for five or more weeks, the great majority of those who used NRT did so for 2 weeks or less. The reported number of cigarettes smoked per day was 14 or less for about 54.5% of the sample. Age was distributed with 11.8% of the sample under 25 years of age, 33% between 25–39 years, 32.3% between 40–54 years and 22.8% 55 years or older. The sample was 76% non-Hispanic white, 11.3% non-Hispanic Black, 7.4% Hispanic and 5% of other race/ethnicity. About 15.2% of the sample did not have a high school diploma, 73.3% had a high school diploma and 11.4% had at least a bachelor's degree. The distribution of family income was skewed such that over a third of the sample had an income of less than $25 000 and less than a 10th of the sample had an income of $100 000 or greater.
Table 1
Weighted sample characteristics and unadjusted smoking cessation rates across categories of each covariate
Table 1 also provides smoking cessation rates across categories of each covariate, indicating bivariate (unadjusted) associations between the covariates and quitting. Cessation rate was 17% in the whole sample. There was very little evidence that method of quit attempt was associated with cessation rate (p<0.074). However, the duration of pharmacotherapy use (p<0.001), number of cigarettes smoked per day (p<0.001), age (p<0.001) and race/ethnicity (p=0.003) were all associated with quitting. Higher socioeconomic status as measured by education, occupation and income, was associated with a higher cessation rate (p<0.001 for all three indicators of socioeconomic status). Sex had no association with cessation.
Adjusted results from multivariable logistic regression models
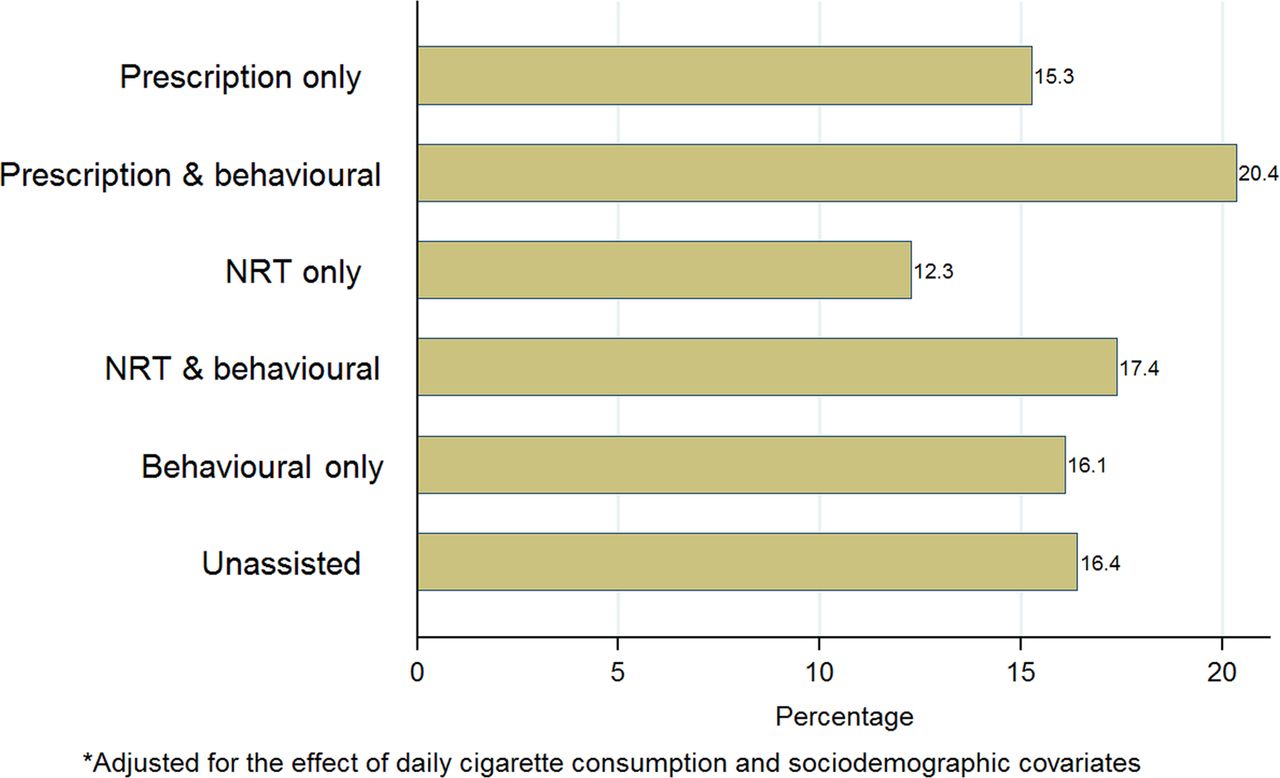
Table 2 provides adjusted ORs for the association of method of quit attempt with the probability of smoking cessation. Figure 1 shows the adjusted cessation rates for various quitting methods. Unlike the unadjusted results in table 1, which provided very little evidence of an association between quitting method and successful cessation, the adjusted results revealed some evidence of an association (p=0.025). The highest cessation rate was among those who used prescription medication and behavioural counselling (20.4%) followed by those who used NRT and behavioural counselling (17.4%), attempted to quit unassisted (16.4%), used behavioural counselling only (16.1%) and those who used prescription medication only (15.3%). The lowest cessation rate was among those who only used NRT as a quitting method (12.3%).
Table 2
Adjusted* ORs and 95% CIs for the association of method of quit attempt and duration of pharmacotherapy use with the probability of successful smoking cessation
Figure 1
Adjusted cessation rate by method of quit attempt.
Table 2 also provides adjusted ORs for the association of duration of pharmacotherapy use with the probability of smoking cessation. Figure 2 shows the adjusted cessation rates for various durations of pharmacotherapy use. Consistent with the unadjusted results in table 1, the adjusted results in table 2 also provide evidence (p<0.001) of an association between duration of pharmacotherapy use and successful cessation. As shown in figure 2, cessation rates were highest among those who used prescription medication for 5+ weeks (28.8%) and those who used NRT for 5+ weeks (27.8%). Cessation rates for those who used prescription medication or NRT for less than 5 weeks varied from 6.2% to 14.5%. Cessation rates for those who used only behavioural counselling and those who attempted to quit smoking unassisted were 16.1% and 16.4%, respectively.
Figure 2
Adjusted cessation rate by duration of pharmacotherapy use.
The results pertaining to the association of other covariates with successful cessation were very similar in the multivariable regression models for method of quit attempt and duration of pharmacotherapy use. These results were consistent with bivariate associations reported above, except for the fact that there was very little evidence for an association of race/ethnicity and smoking cessation in multivariable analyses.
Discussion
This is the first population-based study to examine the association of successful smoking cessation and duration of use of prescription medication as well as NRT for smoking cessation. We found that using pharmacotherapy for 5 weeks or longer is associated with a higher probability of cessation compared to using pharmacotherapy for shorter durations, only using behavioural counselling or trying to quit unassisted.
Our findings are consistent with the results of a study of a hospital-based cessation programme where participants who used NRT for 5 weeks or longer were found to have a higher cessation rate at 6 month follow-up.28 However, our findings are not consistent with those of a population-based study that did not find any evidence that using NRT for more than 6 weeks versus not using NRT at all was associated with smoking cessation.12 In that study, the survey response rate was low, the sample size was small and prescription medications were not examined. These factors could explain the discrepant findings.
While we found that smokers who used pharmacotherapy for at least 5 weeks have a far more favourable outcome than others, only 11% of the sample was in this group and notably about 70% of the sample did not use any pharmacotherapy for smoking cessation. Previous research indicates that barriers to the use of these cessation aids include concerns with their addictiveness, cost and side effects, as well as the belief that no treatment of any kind is needed to quit smoking.29–31
A major limitation of the study is that there is a strong possibility of reverse causation such that relapse would determine duration of pharmacotherapy use rather than vice versa.32 Smokers who use varenicline to quit smoking are asked to completely stop smoking 1 week after their quit date.33 Thus, individuals who use pharmacotherapies and relapse a short while after a quit attempt may stop using these aids. In such cases, an unsuccessful quit attempt would cause a short duration of pharmacotherapy use instead of the reverse. Furthermore, because of its observational nature, our study cannot establish a causal link between the duration of pharmacotherapy use and successful smoking cessation. While our analyses controlled for several important predictors of cessation including daily cigarette consumption, age, race, education, occupation and income, it is possible that there might be residual confounding related to variables such as depression, anxiety, alcohol use and financial stress.34,35 Such confounding would further weaken the ability of the study to imply causation.
Another weakness of the study relates to the fact that smokers forget many quit attempts7,36 and they are more prone to recall attempts that used pharmacotherapy than those that did not.14,17 Such recall bias can underestimate the success rate of attempts at quitting with the aid of pharmacotherapy.17
A strength of this study was that it used a large nationally representative sample with a relatively high response rate. This was the first time that questions about the duration of pharmacotherapy use were included in the TUS-CPS. We know of no other national data on the general population that provide information on this variable. Many population-based studies of pharmacotherapies for smoking cessation have found these aids to be ineffective. It is likely that if these studies were able to account for duration of use, their findings would have been different. However, data on duration of use are not routinely collected and a large sample size would be required to provide a reliable estimate of the effect of using these medications for duration of a few weeks. Nonetheless, it would likely be an important area for further research to establish the relationship between duration of use of pharmacotherapy and successful quitting in the general population.
Our results strengthen the findings of clinical trials about the efficacy of pharmacotherapy for smoking cessation and indicate that these aids might also be successful in the general population if they are used for at least 5 weeks.


No hay comentarios:
Publicar un comentario
Danos tu opinion, enriquece el post.